Image

Allison Kuznitz | SHNS
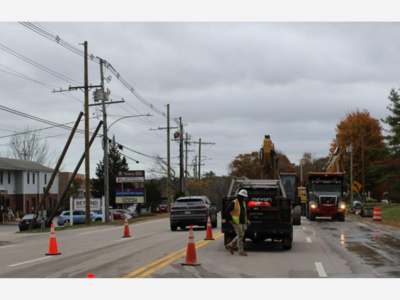
A growing shift of patients receiving care in costlier settings is contributing to the ongoing rise in health care spending.
While average commercial health care spending grew by 8.8% from 2022 to 2024, less than half of that jump was driven purely by price growth, said David Auerbach, the Health Policy Commission's senior director of research and cost trends.
Other factors had an outsized impact, Auerbach said at the agency's annual hearing to help set the health care cost growth benchmark, a data point that has been surpassed for the past four consecutive years.
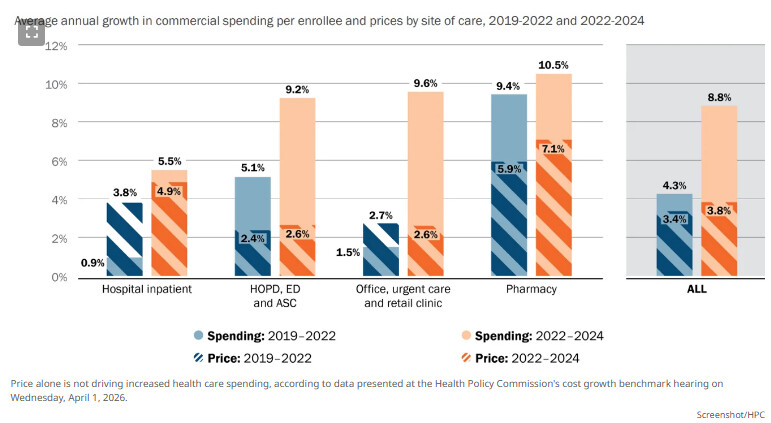
"We see shifts toward higher priced prescription drugs, shifts toward higher-cost imaging modalities, shifts toward higher-cost settings of care for colonoscopy for routine screenings," Auerbach said. "We've reported on increases in C-section rates for low-risk births. And finally, there's rapid growth in a handful of very high-priced procedures."
Colonoscopies on average cost about $2,600 in hospital outpatient settings, compared to $1,600 in ambulatory surgical centers and $980 in office settings. GLP-1 drugs fueled prescription spending growth, as did an increased uptake of drugs that cost more than $1,000 between 2020 and 2024, according to his presentation.
The volume of commercial patients who were admitted in hospitals and classified at the highest severity level nearly doubled from 2016 to 2025, which also led to increased spending. But the trend is more a result of "coding behavior" rather than a surge in patient acuity, Auerbach's presentation said.
As health regulators, lawmakers and business leaders gathered to weigh potential changes to the benchmark — established through a 2012 law that critics say has failed to keep spending at affordable levels — Auerbach highlighted deeply rooted care delivery challenges that are ultimately straining patients' wallets.
Total health care spending per capita grew by 5.7% between 2023 and 2024, while the benchmark was set at 3.6%, a Center for Health Information and Analysis report found last month. Affordability woes are worsening, and more Bay Staters are choosing to delay care due to cost concerns.
The state is at a "breaking point of complete unaffordable health care," said Rep. John Lawn, co-chair of the Joint Committee on Health Care Financing.
"We are all in this together and unless we solve this, we're going to have very dire consequences for our health care market and our ability to provide affordable and accessible health care," Lawn told hearing attendees.
As an "ex-CEO of a medical institution," Health and Human Services Secretary Kiame Mahaniah acknowledged he tried to balance tough budgets by embracing "higher paid things." He led the Lynn Community Health Center for six years and previously was chief medical officer at North Shore Community Health.
"The incentive was to figure out what I am doing that has the highest margin possible so I can keep paying my employees?" Mahaniah said. "So it's not always like a nefarious, sort of price-gouging things. Sometimes, it's just sheer survival, right?"
Auerbach described the dynamic as a "fault of pricing in the system," which can be hard for health care systems to "resist" as they weigh which treatment options are more profitable. That outlook explains why hospitals are closing labor and delivery units because they're a "money loser," Mahaniah said.
Sen. Cindy Friedman, the Senate's health care point person, said policymakers must understand where health care dollars are flowing as Massachusetts braces to federal funding under the One Big Beautiful Bill Act.
"Are they being invested in health care services and workforce that our residents need and deserve, or are our dollars being hid in systems used for profit instead of care, or being put in entities that are costing the most but offering the least?" Friedman asked at the start of the hearing.
Liz Leahy, senior vice president of advocacy and engagement at the Massachusetts Association of Health Plans, said administrative spending is not driving health care costs. She instead pointed to the cost of care, including across hospital outpatient settings and pharmaceutical spending.
"Chemo oncology drugs are one of the fastest growing drivers of cost, now totaling more than $3 billion annually," Leahy said. "And these costs reflect both the price of the drug, which is set by the drug manufacturers, and the price of the site of care set by the providers. And neither of those price components are meaningfully constrained today."
Leahy said hospitals, providers and pharmaceutical manufacturers must work together and be held accountable. Insurance Commissioner Michael Caljouw pointed out that insurers are "uniquely in the middle" of negotiating prices with those other major players.
"We've seen rapid consolidation of health care systems," Leahy replied. "I won't argue whether it's good or bad, but I will let you know that that has significantly reduced the negotiating leverage of health plans across the country and here in Massachusetts."
Retailers Association of Massachusetts President Jon Hurst said Wednesday marks the biggest insurance renewal date of the year for small businesses. A recent member survey found the average premium increase was 13.6%, he said.
Hurst said "something is wrong" with the state's benchmark and the individual health insurance mandate, which top elected state officials plan to celebrate this month on its 20th anniversary.
"As we have stated for many years, small employers need fairness and help on controlling health care and insurance costs," Hurt said in written testimony, as he pointed to an exodus of small group employers leaving the fully insured marketplace and turning to self-insured or partially-self funded plans. The trend, he said, is "an attempt to "mitigate the cost of nearly 60 state mandates."
"Estimates put state mandates and assessments at 17-24% of a fully insured small business’ premium," Hurst added. "For a $47,000 family policy—unfortunately a very real number this year-- that’s $8,000-$11,000 in state mandates."
The HPC board is slated to vote on setting the benchmark on April 16. A decision to change the target could trigger another hearing before the Joint Committee on Health Care Financing.
Alison Kuznitz is a reporter for State House News Service and State Affairs Pro Massachusetts.



Sunny, with a high of 98 and low of 68 degrees. Sunny during the morning, clear overnight.